






EDMA podporuje Světový den tuberkulosy
EDMA supports World Tuberculosis Day - 24 March 2004!
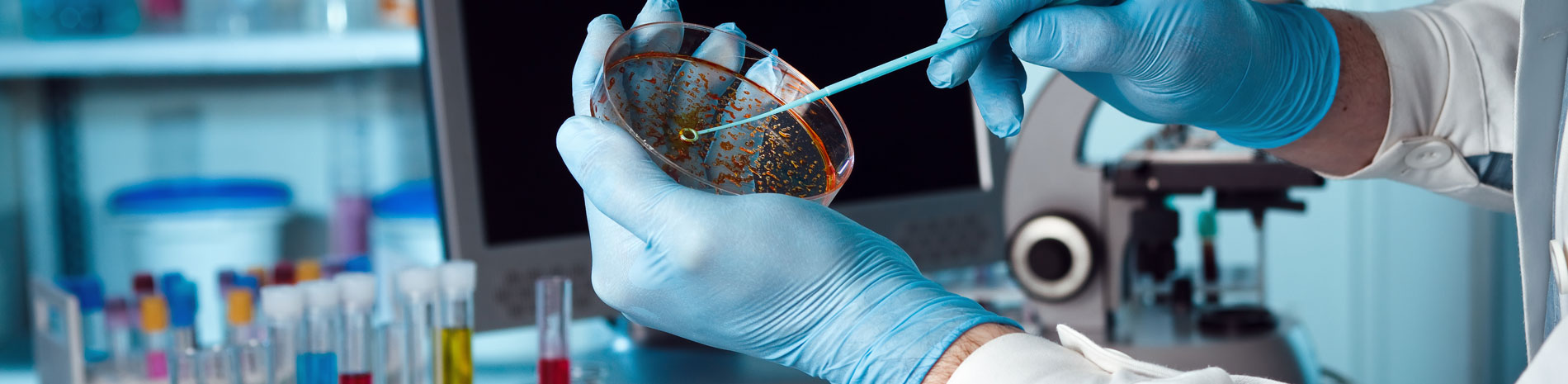
Tuberculosis was easier to control in the past. Today we rely on rapid and accurate detection of TB and drug susceptibility testing.
A third of the world’s population has tuberculosis (TB) and two million people die from TB each year. The risk of disease and drug resistance is increasing as transnational migration brings more people into contact with foreign-borne strains of the bacteria.
EU Expansion
Identifying the problem
Tuberculosis may or may not produce clinical symptoms. Current tests for active TB rely on confirmation of the growth of the bacterium, Mycobacterium tuberculosis, as found in patient sputum samples. Current automated liquid culture methods are able to detect Mycobacterium tuberculosis in positive TB samples in about 10 days. New laboratory tests are continuing to be developed and modified in the hope of diagnosing tuberculosis even faster and in patients that have less obvious clinical symptoms such as those from high-risk patient groups e.g. HIV positive patients.
The spread of TB is linked to the HIV epidemic
HIV has increased the incidence of TB. Out of the 36 million HIV infected persons worldwide, one in three are co-infected with TB. Although it has been shown that TB is a leading cause of HIV-related complications leading to death, HIV and AIDS programmes often do not pro-actively treat for co-infection with TB. Despite close epidemiological links between HIV and TB, public health responses to the two have largely been segregated. Because the burden of TB is so closely linked to the HIV epidemic, prevention of HIV must become a priority for TB programmes, just as TB care and prevention should be a major concern within HIV/AIDS programmes. All individuals with HIV should be routinely tested for TB, and vice versa.
Detect, Contain, Cure
Effective TB control and containment can be achieved by:
1) Efficient, increased screening and diagnosis: Directly related to increased cure rates early, accurate diagnosis of TB combined with appropriately managed treatment can make a vast contribution to the prevention of a TB epidemic.
2) Drug susceptibility testing: As bacterial strains become more and more resistance to standard first-line drugs ensuring the effectiveness of second-line drugs through patient and bacterial testing is crucial for selection of the right initial treatment and quick eradication of the disease. When second-line drugs are required for resistant strains of TB, the cost is approximately 100 times more than treatment using first-line drugs, varying from $2000-$5000 US (Dye & Williams, 2000). Second-line drugs are also more toxic and have more side-effects and it can take much longer to treat a resistant strain of TB.
3) Directly observed therapy (DOT): To guarantee that therapy is taking place correctly, healthcare workers will witness the patient taking their medicine. This not only helps to speed recovery and cure the disease in that individual, the strict treatment regimen also helps to reduce the chance of allowing the bacteria to become resistant to the medication. This method serves to further protect the public and halt the epidemic.
The dangers of multidrug-resistant-TB (MDR-TB): The prevalence of MDR-TB strains are increasing dramatically. Focal points for MDR-TB infections have been identified in:
MDR-TB is highly virulent and remains infectious for longer periods with patients having a much higher risk of death in what should be a curable disease. MDR-TB can be caused by an inadequate treatment regimen, incomplete treatment (non-compliance) and poor case management. Systems that foster adherence to therapy are crucial in beating MDR-TB epidemics.
The globally recognised ‘Standardized Short Course’ treatment of first-line drugs is not effective for MDR-TB. Where MDR-TB is suspected or when there are numerous drug-resistant cases, individuals will require access to reliable laboratory facilities with standardized and proven testing and accurate diagnostic methods. There are established rapid liquid-culture methods for TB detection and drug susceptibility testing as well as molecular/genetic methods for dealing with drug-resistant strains of bacteria. The technical capability of laboratories that have both trained staff and the necessary equipment to perform these tests properly often require additional financial resources to be made available.
“Drug resistance tends to rise when national TB programs do not adhere to international recommendations for TB control.” (Raviglione et al, 2001)
World Health Organisation (WHO) targets
The WHO goal for the control of MDR-TB is to detect and treat 70% of TB patients and of these at least 85% should be cured. Presently the percentages are 37% detection/treatment and 83% cure. These figures demonstrate that there is a long way to go to achieve the necessary detection and correct treatment of TB that will halt the spread of the disease and reverse prevalence rates. Containment of drug-resistance bacterial strains and the interruption of the person to person transmission cycle both result from early and accurate diagnostic testing methods.
Read more:
Ø The Stop TB Campaign (2004). Themes and Strategy. Retrieved from http://www.stoptb.org
Ø EuroTB Country Profiles http://www.eurotb.org/country_pro.htm
Ø Infuso, A., Antoine, D., Barboza, P., Falzon, D. 1999. European Communicable Disease Bulletin – Surveillance of anti-tuberculosis drug resistance in
Ø Infuso, A., Barboza, P., Belghiti, F., Falzon, D. 2003. Recent trends in anti-tuberculosis drug resistance in
References
Ø Raviglione, M., Gupta, R., Dye, C., & Espinal, M. (2001).The burden of drug-resistant tuberculosis and mechanisms for its control. Annals of the
Ø Dye, C., Williams, B. (2000). Criteria for the control of drug-resistant tuberculosis. Proceedings from the
Ø Williams, B., Dye, C. (2003). Antiretroviral drugs for tuberculosis control in the era of HIV/AIDS. Science. Vol. 1.1535-1537.
Other related articles:
Ø Isolation of Mycobacterium nucleic acids (RNA&DNA) from sputum and cultures strains using magnetic silica particles. 12th European Congress of Clinical Microbiology and Infectious Diseases.
Ø Vernet, G., Jay, C., Rodrigue, M., Troesch, A. 2004. Species differentiation and antibiotic susceptibility testing with DNA micro arrays, Journal of Applied Microbiology. 96, 59-68.
Bemer, P., Bodmer, T., Munzinger, J., Perrin, M., Vincent, V., Drugeon, H.